"Restoring Form in Abdominoplasty"
 This article originally appeared in the ISAPS News, January – March 2020
This article originally appeared in the ISAPS News, January – March 2020
Patronella, C.K., Restoring Form in Abdominoplasty. ISAPS News. Volume 14, Number 1, January – March 2020
As plastic surgeons, we strive to provide ideal aesthetic improvements with minimum surgical stigmata. Today, we are more attentive to subtle anatomical details than ever before, incorporating adjunctive techniques, such as facial fat grafting during facelift surgery, to enhance youthful anatomical features. Traditional abdominoplasty often failed to recreate anatomical nuances such as the soft contour valleys of the linea alba and linea semilunaris, resulting in a uniformly, flat-as-a-board and excessively taut abdomen. Today, the more sophisticated, 21st century consumer has available digital multimedia resources from around the globe and has become keenly informed about the details of the procedures we perform and now often rejects less attractive, unnatural changes.
Our group recognized the attractiveness of a detailed treatment of the abdomen with the publication of our paper, Abdominal Etching: Differential Liposuction to Detail Abdominal Musculature in the Aesthetic Plastic Surgery Journal in 1993. In our experience, concomitant liposuction of the abdomen during abdominoplasty increased vascular perfusion complications with the procedure, especially in patients requiring a more comprehensive abdominoplasty for correction of skin redundancy of the upper abdomen. My approach evolved beginning 20 years ago, stimulated by my own dissatisfaction with the uniformly flat and overly tight abdominoplasty that I learned in my training. While most patients didn’t complain, many noticed the unnaturalness, so I supplemented with secondary liposuction to enhance anatomical definition. The procedure I perform today is markedly different, incorporating numerous details and requiring an extra 45 minutes, but vastly more satisfying for my patients and I. The two most impactful maneuvers in this abdominoplasty, direct differential sub-Scarpa’s fat thinning and Anatomy Defining Progressive Tension Sutures, are combined to create a more authentic, toned abdomen.
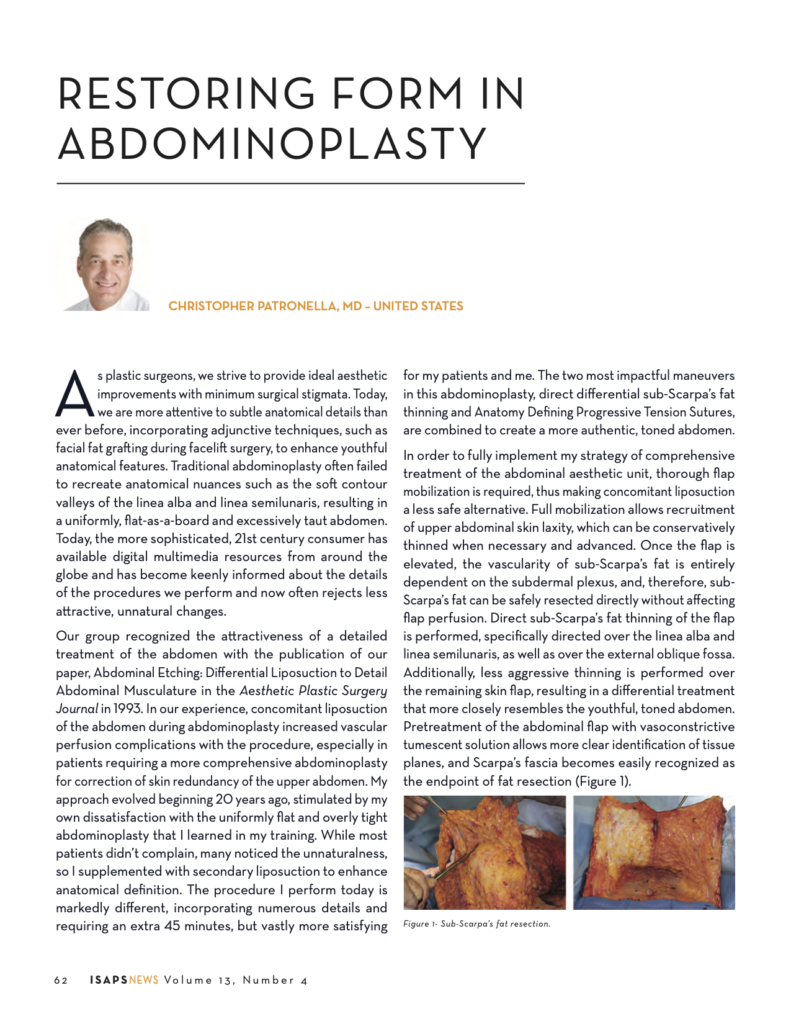
In order to fully implement my strategy of comprehensive treatment of the abdominal aesthetic unit, thorough flap mobilization is required, thus making concomitant liposuction a less safe alternative. Full mobilization allows recruitment of upper abdominal skin laxity, which can be conservatively thinned when necessary and advanced. Once the flap is elevated, the vascularity of sub-Scarpa’s fat is entirely dependent on the subdermal plexus, and, therefore, sub-Scarpa’s fat can be safely resected directly without affecting flap perfusion. Direct sub-Scarpa’s fat thinning of the flap is performed, specifically directed over the linea alba and linea semilunaris, as well as over the external oblique fossa. Additionally, less aggressive thinning is performed over the remaining skin flap, resulting in a differential treatment that more closely resembles the youthful, toned abdomen. Pretreatment of the abdominal flap with vasoconstrictive tumescent solution allows more clear identification of tissue planes, and Scarpa’s fascia becomes easily recognized as the endpoint of fat resection (Fig 1).
An anatomy-defining application of progressive tension sutures (PTS) requires placement in a specific pattern aimed to enhance muscular definition (Fig 2). Stabilizing the skin flap with PTS prevents serous fluid collection and bursa formation, preventing a blunting effect along these fascial zones of adherence. Stabilizing the flap with PTS splints the subcutaneous-fascial interface along the linea alba, linea semilunaris and over the external oblique fossa, promoting scar tissue adherence during the healing process (Fig 3). With a properly performed PTS technique, drains are not needed, adding comfort and convenience for patients, and enhancing the surgical experience. Differential fat thinning combined with reestablishing zones of adherence produces lasting abdominal wall definition which becomes more distinct, gradually, over a six-month period following surgery. Long term follow up with patients undergoing this procedure has consistently demonstrated maintenance of anatomical definition in those who also maintain stable weights (Fig 4).
In summary, a positive patient experience and good outcomes are critical to a high level of patient satisfaction. The techniques I’ve described are a major component of my overall strategy for enhancing abdominal wall definition during abdominoplasty (1), providing a more authentic-appearing outcome and, as a result, improving patient satisfaction. Other important steps such as detailed treatment of the mons and umbilicus, which are beyond the scope of this review, are covered in the original article with accompanying procedure video in the Aesthetic Surgery Journal in November/December 2015 (1).
Reference:
- Patronella, CK. Redefining Abdominal Anatomy: 10 Key Elements for Restoring Form in Abdominoplasty; Aesthetic Surgery Journal 2015, Vol 35(8) 972–986;